02 Mar Cardiac Part 2
Right Ventricle/Pulmonary Embolism, Pericardial Effusion & Cardiac Tamponade
Indications:
Evaluating cardiac function, including undifferentiated dyspnea, chest pain, heart failure and shock – Expanded to include evaluation for massive pulmonary embolism, pericardial effusion and cardiac tamponade.
Probe Choice:
Phased-array.
For cardiac applications, the ultrasound indicator is on screen right, which is opposite that of standard ultrasound applications.
Basic Views & Anatomy: See Cardiac Part 1
Pathology:
Pulmonary Embolism with Right Heart Strain:
Right Ventricular Enlargement:
Parasternal long axis view showing the RV very much enlarged compared to the aortic outflow track & left atrium (typically in this view they are 1:1:1).
This apical 4 chamber view shows that the RV is close to 1.5x the size of the LV. A good rule of thumb is that the RV should be smaller than the LV, and if they are equal size then there is RV strain.
D-Sign:
Normal parasternal short axis for comparison:
D-sign:
In this parasternal short axis, we see the right ventricle overriding the left ventricle, pushing the septum and forcing the left ventricle into a “D” shape, hence the name: the D sign.
Apical 4 chamber for comparison:
McConnell’s Sign:
This sign is caused by akinesis of the free wall of the right ventricle, with resulting relative hyperkinesis, or exaggerated movement of the apex of the right ventricle. This is a sign of right ventricular strain, and is commonly associated with acute pulmonary embolism.
Pericardial Effusion:
You can see pericardial effusion in any standard views. However, certain views are more high yield than others. Namely, the parasternal long axis and subxiphoid views.
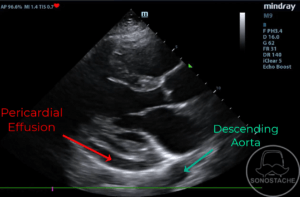
Parasternal long axis with pericardial effusion:
There is an anechoic fluid collection tracking down behind the left ventricle, but between the myocardium and the descending aorta. This is key as it differentiates it from a pleural effusion (which will track posterior to the descending aorta).
Subxiphoid view with pericardial effusion:
Anechoic fluid collection surrounding the entirety of the myocardium, indicating pericardial effusion. Prominent pericardial fat pad is noted in the near field.
Cardiac Tamponade:
When a pericardial effusion accumulates significantly to cause impaired diastolic function (filling of the heart) it is termed cardiac tamponade. Do not let the size of the effusion fool you, as relatively small effusions may precipitate tamponade physiology if they accumulate rapidly and the heart has not had time to compensate.
Here we see right ventricle diastolic collapse. When the heart should be filling (diastole) the RV is instead collapsing from the pressure related to the pericardial effusion.
Subxiphoid view with RV diastolic collapse.
Pearls:
Patient Movement: The parasternal and apical views may be facilitated by having the patient roll onto their left lateral decubitus position, as well as raising their left arm above their head. This causes the heart to shift more towards the chest wall, and opens the rib spaces.
Pitfalls:
Do not confuse pericardial effusion and pleural effusion. Use descending thoracic aorta to distinguish the two. Pericardial effusions are anterior to the descending aorta, while pleural effusions are posterior.