29 Jan Cardiac Part 1
Basic Cardiac Views, Left Ventricular Function, and IVC
Indications:
Evaluating cardiac function, including undifferentiated dyspnea, chest pain, heart failure and shock.
Probe Choice:
Phased-array.
For cardiac applications, the ultrasound indicator is on screen right, which is opposite that of standard ultrasound applications.
Basic Views & Anatomy:
Parasternal Long Axis:
Parasternal, with indicator towards the patient’s right shoulder:
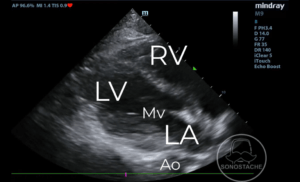
Labeled here from top to bottom we have the right ventricle (RV), left ventricle (LV), mitral valve (Mv), left atrium (LA), and descending aorta (Ao) in cross section. The descending aorta is an important anatomic landmark as this should be the bottom, or back wall of the image. Pericardial effusions will track between the heart and the descending aorta, while pleural effusions will be posterior to the aorta.
Parasternal Short Axis:
Rotate the probe so the indicator is to the left shoulder:
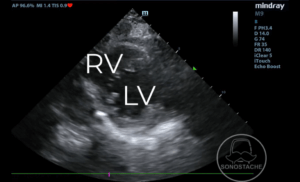
The short axis view cuts the LV (left ventricle) and RV (right ventricle) into cross section.
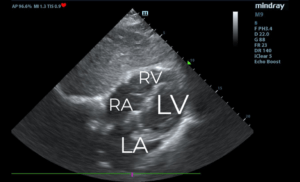
Apical 4 chamber view:
Rotate the indicator towards the patient’s left, and slide the probe to the apex of the heart (4th or 5th intercostal space, anterior axillary line):
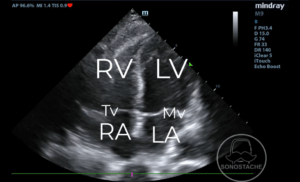
You will see the LV (left ventricle), RV (right ventricle), LA (left atrium), and RA (right atrium) with the septum of the ventricles down the middle of the image. In between the LA / LV will be the Mv (mitral valve) and similarly the Tv (tricuspid valve) in between the RA / RV.
Subxiphoid:
Keep the indicator towards the patient’s left, and move the probe underneath the patient’s xiphoid process (hence the name sub-xiphoid).
Here we can see a similar 4 chambered view. The LA (left atrium), LV (left ventricle), RA (right atrium), and RV (right ventricle). Be sure to decrease the depth enough to see the full heart, as there may be pericardial effusion in the posterior aspect of the image behind the LV.
IVC View:
Center the image on the right atrium, and turn the probe so the indicator is up towards the patient’s head. This will produce an image of the IVC in long axis. You may need to slightly adjust the angle of the indicator to get the IVC in long axis as the IVC itself is often not perfectly angled towards the patient’s head.
Note the mid-range IVC with respiratory variation. On the exam, this is likely to be a euvolemic patient.
Pathology:
Decreased Left Ventricular Function:
Here the left ventricle is hardly squeezing (decreased ejection fraction), along with left atrial dilation and decreased movement of the mitral valve.
Plethoric IVC:
This IVC is plethoric, or plump, with minimal respiratory variation. On the test, this will likely be associated with cardiac tamponade or volume overload.
Collapsible IVC:
Here we see a completely collapsible IVC with respiratory variation. On the examination this will likely be associated with volume depleted states, such as dehydration.
Artifacts:
Unlikely for the exam to test you on artifact directly related to echocardiography.
Pearls:
Patient Movement: The parasternal and apical views may be facilitated by having the patient roll onto their left lateral decubitus position, as well as raising their left arm above their head. This causes the heart to shift more towards the chest wall, and opens the rib spaces.
Inhalation / Exhalation: For parasternal / apical views, you may ask the patient to briefly exhale and hold in end-expiration to decrease the lung expansion which may obscure your vision. The subxiphoid view may be facilitated by holding inspiration, which causes the diaphragm to push abdominal contents out of the way. Don’t let the patient hold their breath too long!
Liver as an echogenic window: For the subxiphoid view, you may slide the probe towards the patient’s RUQ by a few centimeters, which may allow you to use the liver as a window to the heart.
Pitfalls:
Ensure you increase the depth appropriately to view the entirety of the heart in all views.
Don’t mistake the aorta for the IVC. The aorta will run posteriorly to the heart, while the IVC drains directly into the right atrium.
Aorta in long axis, not to be mistaken for the IVC.